Front:
63
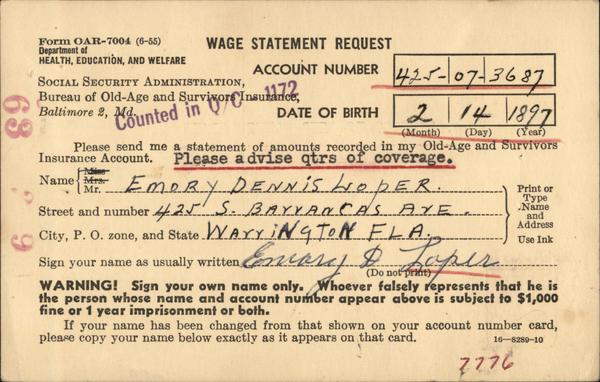
Form OAR-7004 (6-55)
Department of
HEALTH, EDUCATION, AND WELFARE
WAGE STATEMENT REQUEST
ACCOUNT NUMBER 425-07-3687
SOCIAL SECURITY ADMINISTRATION,
Bureau of Old-Age and Survivors Insurance,
Counted in or
Baltimore 2, Md.
Miss
Name Mrs.
Mr.
DATE OF BIRTH
2 14 1897
(Month)
(Day)
(Year)
Please send me a statement of amounts recorded in my Old-Age and Survivors
Insurance Account. Please advise qtrs of coverage.
EMDBY DENNIS HOPER.
Street and number 425 S. BAYYANCAS AYE
City, P. O. zone, and State WAYYINGTON FLA.
Eemary Po
Roper
Sign your name as usually written,
WARNING! Sign your own name only. Whoever falsely represents that he is
the person whose name and account number appear above is subject to $1,000
fine or 1 year imprisonment or both.
(Do not print)
Print or
Туре
Name
Use Ink
If your name has been changed from that shown on your account number card,
please copy your name below exactly as it appears on that card.
7776
16-8289-10
Back:
Your Social Security Account
If you want a statement of
NSACOL
your Federal Old-Age andk FEB"*
Survivors Insurance Account
fill out the other side of this
card.
6-PM
969
Be sure to give your name
and account number exactly
as they are shown on your
account number card, in order
to make sure your account is
properly identified.
If you
have more than one account
number, give all of them.
It is not necessary for you
to pay anyone to aid you in
securing this information.
There is no charge for this
service.
Be sure to place a stamp
on this card before mailing
it to us.
COLA,
(..
NEW HOPE FOR HEARTS
-SUPPORT
GPO 16-8289-10
THE HEART
SOCIAL SECURITY ADMINISTRATION,
CANDLER BUILDING,
BALTIMORE 2, MD.
LINCOLN

{kind=link}